
Distance Learning: Anemia
Objectives
Review the physiology and pathophysiology of RBCs
Create a differential for different subsets of anemia
Apply your anemia framework to the cases below
Theory
Additional Resources


Above is another curbsiders podcast on anemia, what can we say, they do a good job. To the right is a review article from the Mayo clinic which is worth a read, it is a tad long, but set aside 45 minutes this week to read through it, it’s worth it. Finally, Tarun has found a collection of cool mnenomics from #EM3, see below:

Cases
Case 1: You are seeing a 42 y/o African American male in clinic who has a history of HTN and severe recurrent back pain. Events occur one to two times a year, no clear precipitants, are severe without any alleviating factors. They usually last a few days and resolve with analgesia. Initial and follow up labs are below:

MCV 70.8 LDH 615 Hgb A 20.1
RDW 16.8 Haptoglobin <30 Hgb A2 5.4
Fe 102 Hgb F 4.5
Ferritin 380 Hgb S 70.0
TIBC 281
How do you interpret the labs and Hgb Electrophoresis above? Discuss your impression of this patient.
Case 2: A 77 y/o male with no major past medical history presents with progressive fatigue and shortness of breath. His symptoms have had a gradual onset over the past 2 months. He reports an unintentional 10 lb weight loss over this time period. ROS is negative for chest pain, orthopnea, edema, abdominal pain, and melena. He is a non-smoker, and only takes a multi-vitamin daily. Physical exam is noteworthy for lymphadenopathy.
Blood Pressure: 126/78
Heart Rate: 76
Respiratory Rate: 19
SpO2: 98%
CBC 1 year prior:
Additional Labs: LDH 405, haptoglobin < 30, Reticulocytes 5%,
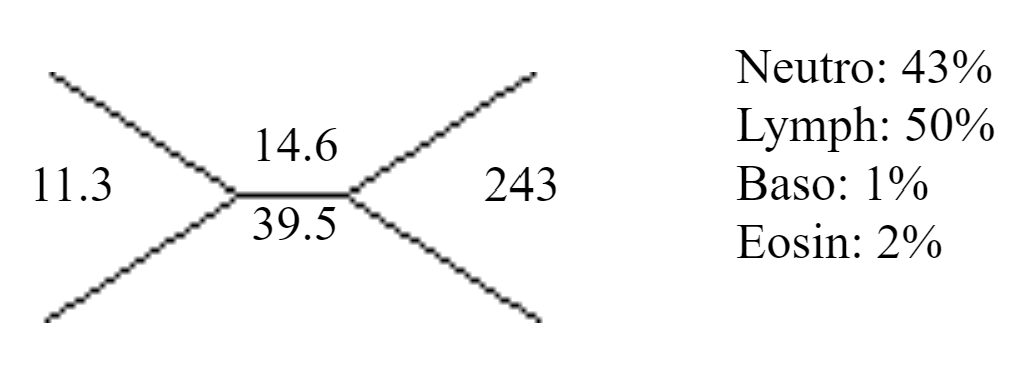
CBC On Admission:


Describe how you go about making your differential diagnosis for this patient?
Case 3: The ED is calling up a patient for a night admission. The patient is a 53 y/o M with a history of HTN (HCTZ, Lisinopril and Amlodipine), GERD (Ranitidine), and Chronic Anemia (Baseline Hgb ~11) who presents after several days of worsening epigastric abdominal pain for which he took increasing amounts of ibuprofen, melena and hematemesis that began just prior to presentation. He has not tolerated any PO including medications in the last 2 days. Below are his labs and vitals.
Blood Pressure: 110/75
Heart Rate: 103
Respiratory Rate: 22
SpO2: 98%

How concerned are you about this patient? Discuss his history, vitals, and labs.
Case 4: You admitted a patient with a history of cirrhosis due to autoimmune hepatitis now 1 year post liver transplant on tacrolimus, cellcept and 5mg prednisone who presented with abdominal pain, diffuse diarrhea, and severe acute kidney injury. Work up revealed confirmed CMV viremia, colon biopsy showed CMV colitis and he was started on IV Ganciclovir with improvement in his symptoms. CBC showed worsening anemia, leukopenia, and thrombocytopenia. LDH was mildly elevated to 452, haptoglobin was < 30, and bilirubin was normal. Slide is below.
What do you see on this slide? Discuss you impression of the patient and how the peripheral blood slide?
MKSAP 18
Heme Onc 4
Heme Onc 43
Heme Onc 59
Heme Onc 65